The History of the PolyVent Educational Platform

The PolyVentilator - A Response to the Covid-19 Pandemic
The novel coronavirus (SARS-CoV-2) swept around the globe, infecting millions of people in nearly every country. The disease onset, also known as COVID-19, has a range of possible negative health impacts including pneumonia and even lung damage.
The most severe cases require clinical intervention. This was typically provided through continuous positive airway pressure (CPAP) machines and even invasive ventilation to ensure the patient could receive enough oxygen despite associated edema. Although it is only a small percentage of patients that require these extreme measures, the rapid rate of transmission of the viral load created situations whereby normally adequate ICU and ventilator capacities were overwhelmed, and patients could not get access to this life-saving therapy.
Because modern ventilators are complex, highly-regulated and expensive devices, their manufacture cannot be quickly scaled to meet this high demand in time to be effective. Their production is centralized and controlled by several key market players who compete using incremental technological improvements. This fact alone created several problems regarding accessibility of available products. Equally problematic was the fact that the component parts of ventilator systems were in short supply since the entire medical supply chain had been stretched by the pandemic. Additionally, intellectual property, distributorship, repair and other legal impediments obstructed scaling the manufacture of ventilators or their component parts.
The Open-Source Response to a Ventilator Shortage
The community response to this crisis consisted of students, tech companies, and others attempting to develop ‘ad-hoc’ ventilators to try and bridge known gaps. In addition, to help solve the problem, special regulatory provisions were introduced to ease the minimal standards for “pandemic ventilators.” To date, none have been widely adopted for several reasons. First, many use ambu-bags and other equipment sourced from the same stretched medical supply chain and thus are unable to get parts. Second, clinical data has shown that patients with severe COVID-19 pneumonia have very fragile lungs. Thus, improper ventilation can cause significant additional damage, worsening the outcome for the patient rather than aiding their recovery. As well, most of the ad-hoc ventilators proposed to date lack the fine control, measurement and feedback systems required to ensure they are not injurious to patients, and have thus not been adopted by the medical community.
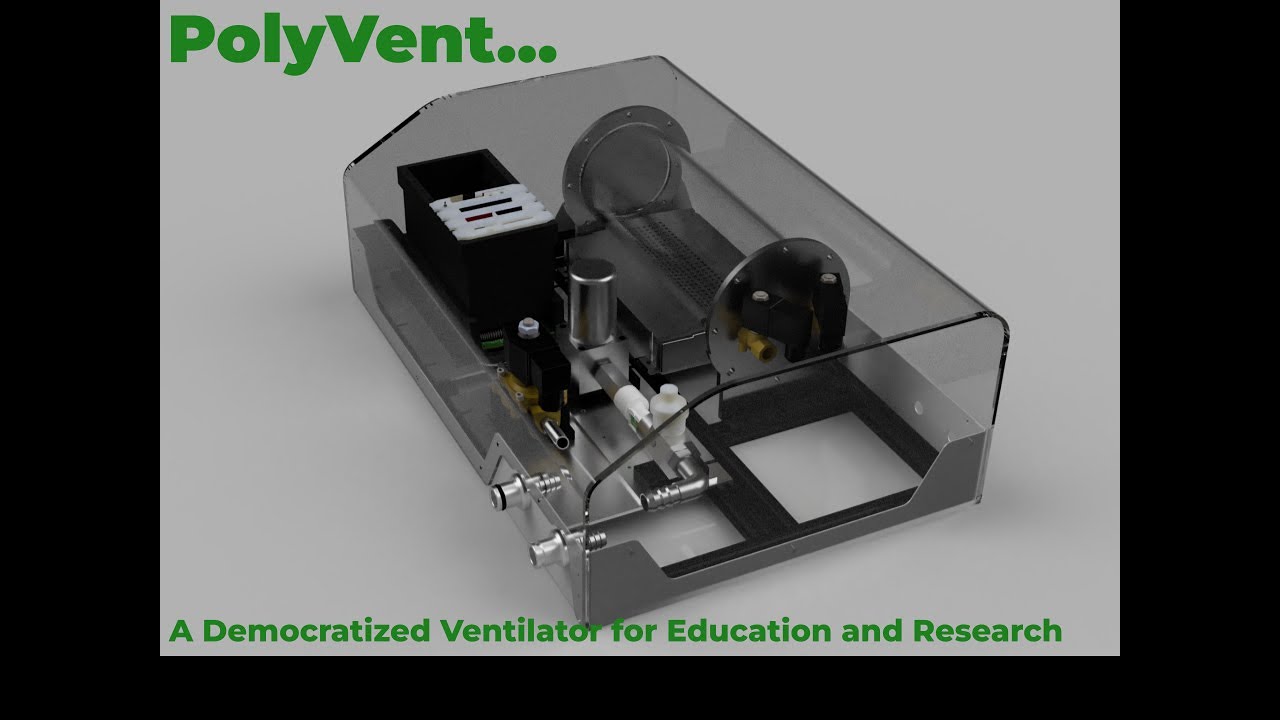
In response to these limitations and the needs of the crisis, Public Invention created the PolyVent: an open-source, modular ventilator meant for research and educational uses and to combat the shortage of related medical devices.
PolyVent contributors include: Shaili Arjani, Nathaniel Bechard, Brandon Beierle, Austin Campbell, Pierre-Luc Charron, Rui Couto, Lukesh G. Dhangaonkar, Joodi Mourhli, Alisa Nussbaumer, Santosh Roy, Levi Türk, Sujay Umarjikar, and Antal Zuiderwijk.

The Story of the PolyVent
PolyVent is a diverse volunteer team of international engineers, scientists, clinicians and other professionals who have joined forces to design, build and produce a clinical-grade, open-source ventilator in response to the COVID-19 crisis and the resulting global shortage of ventilators.
Our approach is one of flexibility, with a modular design that allows modification of parts or whole modules to accommodate local supply chains and part availability. Our system software can be calibrated to account for changes in key system parameters, allowing each ventilator to function as designed, even if the component parts are different from the reference specification.
Working with clinicians, we have also focused on ensuring PolyVent meets the complex clinical needs of COVID-19 patients, as well as having the flexibility to be used for treating other conditions, such that we maximize it’s efficacy now, and also leave a lasting legacy of equipment that can be used beyond the pandemic. As part of our design process, we have undertaken rigorous design reviews to ensure patient safety at every step, engineering failsafe protective features in each module. We are also planning to create VentCloud, a cloud-based data aggregation tool that will collect and analyze performance data from each PolyVent ventilator to identify failure modes, performance enhancements, and with clinician support, patient outcomes.
We realized early on that designing a ventilator, while a significant task in itself, is only half the battle. It needs to be able to be produced in the countries in which it will be used, both for logistical reasons, as well as to generate local economic benefits and create national pride. It also needs to be accepted by the medical community to be used and needs to be produced to proper quality standards by organizations looking to help rather than profiteer. Accordingly, we have designed an organizational structure built around country Clusters, which will have a leader in each target country, as well as, supply chain, clinical, manufacturing and other personnel as needed. In this way we create a presence in each country PolyVent is deployed to, taking advantage of local knowledge and networks.
Challenges that inspired us:
- Global shortage of ventilators due to the COVID-19 pandemic is causing preventable loss of life.
- Limited ventilator supply as the existing clinical ventilators are too complicated to manufacture, and improvised ones do not conform to the minimal clinical standards.
- Most of the ad-hoc ventilator designs do not meet the minimal standards or are non-scalable.
- We need alt-routes for acquiring ventilator components as the medical device manufacturers and supply chains are strained and broken at many places.
- We are facing an unprecedented crisis of our lifetime. We need to revise our production strategy to solve the logistical imbalance.
- Lack of timely delivery due to entrenched bureaucracy, IP and distributor/repair issues.
- Difficulties in global R&D aggregation and adoption into production.
PolyVent operates like a bridging initiative between multiple semi-autonomous geographical clusters, centred around one adaptable design blueprint. The idea is to allow creation of locally tailored variants of the ventilator, to increase chances of it getting to actual patients.
Check out our media coverage:
Of particular interest is this article by the EU Open Source Observatory.
The PolyVent Project has evolved into the PolyVent Educational Platform, now a product sold here at Public Invention, with a reduced team.
The PolyVent in 2022
In the beginning of 2022, we were having significant mechanical problems with the bellows. Dr. Erich Schulz convinced us to switch to using compressed air and compressed oxygen (at about 50 psi) because they represent a valuable store of energy. We therefore redesigned the PolyVent to use a proportional valve, which we had seen done very successfully in the SmithVent ventilator made by Smith College.
Nathaniel and Antal redesigned the system to make a proportional valve system. It was fully functional and reliable for the first time. However, we continued to improve it.
We made three improvements:
- We redesigned the system to use a single level footprint that made it lighter.
- We replaced the heavy solenoid valve with smaller solenoids.
- We found a better sized proportional valve.
In a major innovation, we switched to a "cake dome" design with an easily removable transparent cover.
In December 2022, we did a 3-hour extra credit module to 12 students in a biomedical engineering troubleshooting class for seniors, which was very well received.

The PolyVent in 2024
At the University of Colorado Boulder / Colorado Mesa Partnership Program, eight senior mechanical engineering students recreated the PolyVent as part of an elective course in Bioengineering in November 2024. With the help of instructors and PolyVent inventors, they implemented all valves, sensors, and other electronics to great success.
Students also generated corresponding files and instructions.
This class project was incorporated as part of a module on pulmonary biomechanics and mechanical ventilation. It will be built upon in future years, as the instructor of the course aims to modify the ventilator for research purposes.
Public Invention continues to provide the PolyVent for similar educational and research opportunities. If interested in accessing the PolyVent or the Polyvent Educational Platform for a similar project, please contact Robert Read at read.robert@gmail.com.